여성형 유방 (Gynecomastia) 에 대한 메모, 약물에 의한 여성형 유방, 원인 약제 목록, 여성형 유방의 grade
여성형 유방 (Gynecomastia) 에 대한 메모, 약물에 의한 여성형 유방, 원인 약제 목록, 여성형 유방의 grade
참고문헌 : Sao Paulo Med J. 2012; 130(3):187-97
여성형 유방의 기전
남성 유방조직은 에스트로겐과 안드로겐의 protein receptor 를 가지고 있다.
에스트로겐은 mammary ductules 를 proliferation 시키고
안드로겐은 이 작용을 억제한다.
이러한 호르몬의 불균형이 여성형 유방을 만드는 주된 기전이다.
estrogen/androgen 불균형 원인 : estrogen 이 증가할 때
(1) 고환이나 부신에서 분비되는 free estrogen level 이 증가
(2) extraglandular aromatization of estrogen precursors
(3) decreased estrogen degradation
(4) exposure to estrogen-like chemicals or exogenous estrogens
(5) use of drugs that cause displacement of more estrogen than androgen from sex hormone-binding globulin (SHBG)
estrogen/androgen 불균형 원인 : androgen 이 감소할 때
(1) decreased androgen production in the testes
(2) increased binding of androgens (relative to estrogens) by SHBG
(3) altered androgen metabolism
(4) drug-induced displacement of androgens from their receptors
(5) androgen receptor defects
남성은 testes 에서 circulating testosterone 95% 를 분비 (estradiol 15%, estrone 5%) 한다.
정상 남성에서 estrogen 의 혈중 농도는 매우 낮다. 대부분의 estrogen 은 (80%) two precursors (androstenedione, testosterone)에 의한 peripheral conversion 으로 생성되는데 각각 estrone, estradiol 이다. (aromatase 가 작용한다.) Peripheral conversion 은 intramammary 와 subcutaneous fat 에서 주로 발생하나 liver, skin, muscles, kidneys 에서도 일어난다. Aromatase activity 는 나이가 많아질수록, BMI가 증가할 수록 커진다.
대부분의 여성형 유방을 가진 남자 환자들은 serum prolactin levels 이 높지는 않다.
또한 hyperprolactinemia 라고 해서 전부 여성형 유방이 생기는 것도 아니다.
여성형 유방의 원인
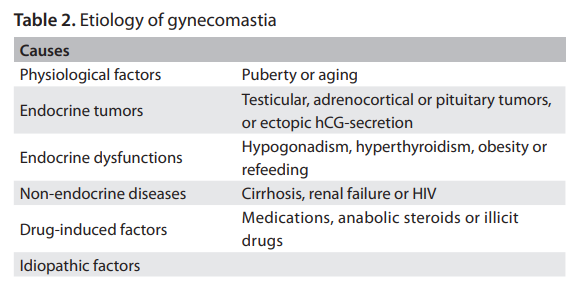
Pubertal Gynecomastia
Mild degrees of pubertal GM generally appear at 13 or 14 years of age, last for 6-12 months and then spontaneously regress in 95% of the cases. The glandular enlargement may be asymmetric and tender.
Relative excess of serum levels of estrogens compared with androgens is implicated in the pathogenesis, due to estradiol production rising sooner than testosterone production.
Aging Gynecomastia
Older men over the age of 65 years often present relative hypogonadism with a decline in plasma testosterone levels, elevation of SHBG and decrease in free testosterone. Furthermore, there is progressive adiposity favoring peripheral aromatase activity. Several comorbidities may be common at this age,
and any medication used may contribute towards provoking or aggravating gynecomastia
Endocrine tumors
(1) Benign testicular tumors (Sertoli or Leydig cell tumors)
Benign testicular tumors (Sertoli or Leydig cell tumors) may secrete estradiol. Secondary suppression of LH levels interferes negatively with testosterone synthesis. The elevated estrogen levels raise the serum concentration of SHBG, which preferentially binds testosterone, thereby lowering the free testosterone levels.
(2) Choriocarcinoma and other germ cell tumors
Choriocarcinoma and other germ cell tumors produce hCG and stimulate testicular cells (Leydig) to secrete estradiol, and furthermore, often cause GM. These tumors may be palpable or be detected only by means of ultrasound. Other hCG secreting tumors of ectopic origin may lead to GM (e.g. carcinomas of the lungs, liver, stomach and kidneys)
(3) Pituitary adenomas
Pituitary adenomas producing prolactin (prolactinomas) may also induce GM.
(4) Adrenocortical tumors
Adrenocortical tumors are generally large malignant types of neoplasia, with predominant incidence in young and middle-aged men. They are feminizing tumors with direct secretion of estrogens and steroid precursors, like androstenedione. The serum estrogen elevation also suppresses LH-mediated testosterone production.
Endocrine dysfunctions
(1) Severe hyperthyroidism
Severe hyperthyroidism increases serum SHBG. Since estradiol
binds less avidly to SHBG than does testosterone, there appears to
be an increase in the ratio of free estradiol to free testosterone, thus
resulting in clinically evident GM in 10 to 40% of the patients.
(2) Primary gonadal failure
- testicular trauma, chemotherapy, mumps, orchitis, leprosy
- Klinefelter syndrome
- Male pseudohermaphroditism with Morris syndrome
- long-standing type 1 diabetes (diabetic mastopathy)
- metabolic syndrome
- refeeding after severe starvation
- substantial weight loss
- functional hyperprolactinemia
Primary gonadal failure as a result of testicular trauma, chemotherapy, mumps, orchitis and leprosy can cause GM by lowering the serum testosterone levels, inducing elevation of LH and stimulating the remaining Leydig cells to secrete estrogens.
Klinefelter syndrome is a chromosomal disorder (47 XXY karyotype) associated with hypogonadism and infertility; in these men, GM is seen in almost 70%. The reason why the presence of an extra X chromosome is linked to GM is unclear.
Male pseudohermaphroditism with Morris syndrome (testicular feminization) is often associated with normal female breast appearance due to gonadal estrogen production. Low testosterone and
elevated LH levels indicate primary hypogonadism. Findings of low testosterone levels with normal LH assays denote secondary testicular failure
It is noteworthy that men with long-standing type 1 diabetes may develop diabetic mastopathy, presenting hard diffuse enlargements of one or both breasts.
Other endocrine-metabolic conditions related to the development of GM include metabolic syndrome, refeeding after severe starvation and substantial weight loss and functional hyperprolactinemia.
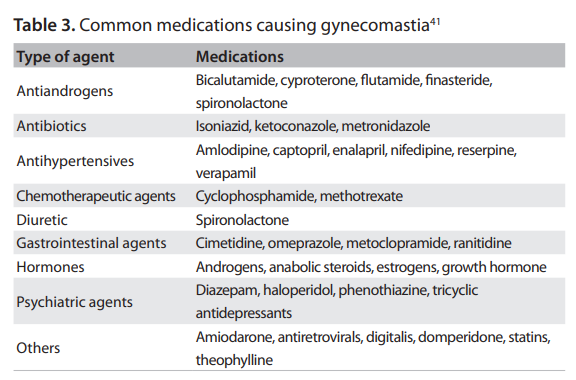
약물로 인한 여성형 유방
One of the medications most frequently associated with GM is the diuretic spironolactone, which is a competitive antagonist of aldosterone. Spironolactone also inhibits testosterone production in the testes, enhances the aromatization of testosterone to estradiol and binds to androgen receptors in some tissues,
thereby acting as an antiandrogenic substance.
Androgen deprivation therapy for prostate cancer frequently presents GM as a side effect. The incidence of GM depends on the type and duration of the hormone therapy, but it can be as high as 40-70%
Some illicit drugs, such as cocaine, heroin and amphetamines, and other abused drugs, are commonly associated with GM. Marijuana is believed to interfere with estrogen receptors and acts as a phytoestrogen
Doping with anabolic androgenic steroids, gonadotropins and growth hormones for power sports and weight training is rampant. In male athletes, these iatrogenic drugs may suppress spermatogenesis and/or induce GM.
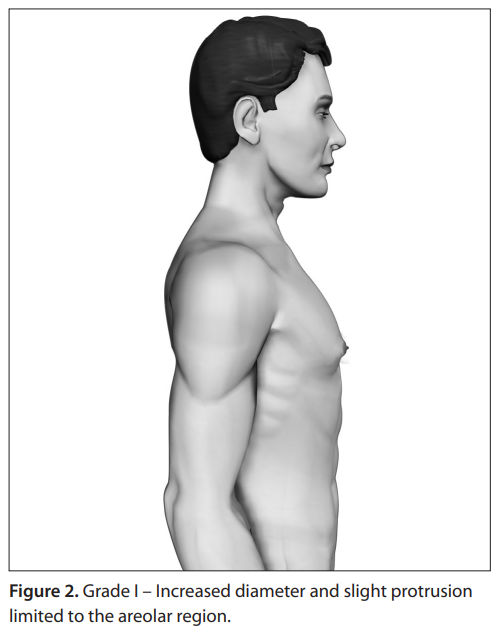
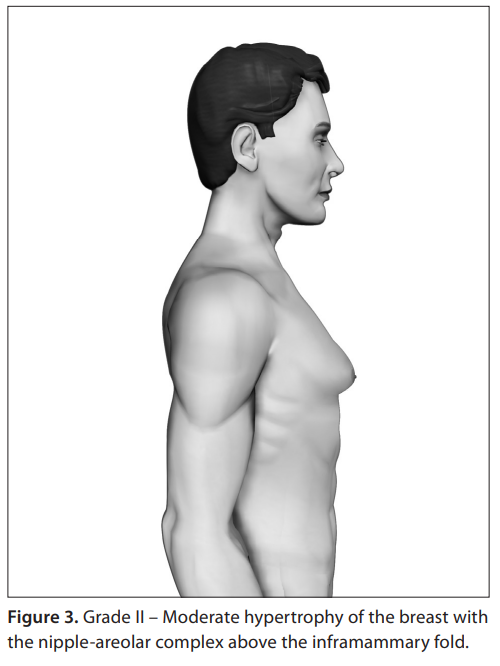
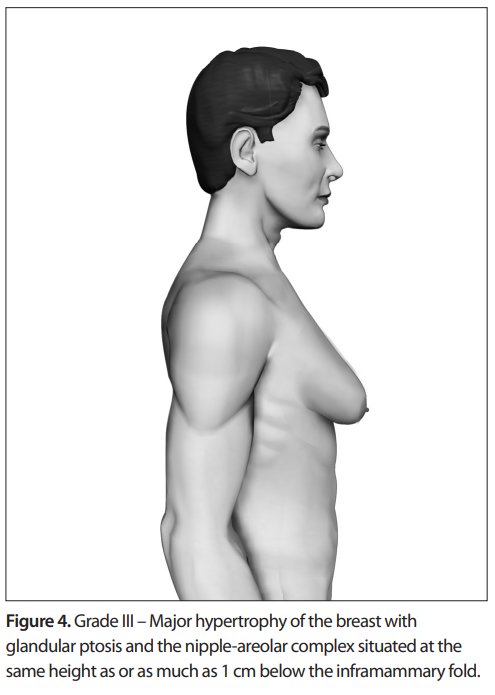
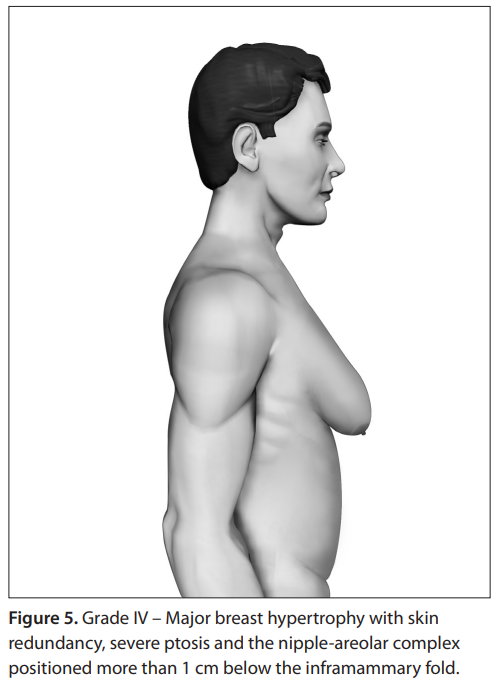
여성형 유방의 중증도 분류