Probe maker 의 위치 약속
환자가 누워있을 때는 marker 가 오른쪽, 머리쪽으로 방향을 두는 것이 원칙이며, 엎드려 있을 때는 왼쪽, 머리쪽으로 방향을 둔다.
Normal sonographic findings of kidney
신장 실질의 두께는 약 1~2cm 정도이며, 1cm 미만일 경우 CKD가 의심되는 소견이다. Renal pole 의 실질 두께는 다른 부위보다 두꺼우며, 신장의 크기는 연령, 성별, 신체 체형, 특히 키, 수분 상태 등에 따라 차이가 난다. (renal 의 upper pole 이 posteromedial 방향으로 놓여 있다.) 정상 성인의 신장 장축길이는 9~12cm 정도 이며, 단축 길이는 5-6cm, 두께는 3-4cm 정도이다. 만약 신장의 길이가 8~9cm 정도라면 그 환자의 키가 작은 것은 아닌지 pheotype 을 살펴보아라. 8cm 이하로 크기가 작을 경우 CKD 일 것이다. (cortex, medulla 모두 얇아져있으며, cortex 의 밝기가 밝다.) 좌측 신장이 우측보다 크며 좌우 신장의 차이는 약 1.5~2.0cm정도 이다. (한국의 경우 우측 10cm, 좌측 10.5cm), 양쪽 신장 크기 차이가 2cm 이상이라면 considered significant discrepancy 가 있다고 볼 수 있으며 추가적인 평가가 필요하다.
*후려치기
- 신장의 장축 크기 8~12cm,
- 좌측 신장이 우측보다 크다. (2cm 미만 차이)
- cortex 는 1cm, cortex, medulla 포함한 실질은 2cm 두께 (반반)
Capsule 의 경우 초음파에서 hyperechoic 하며 하얗게 보인다.
Cortex 는 1cm 이상의 두께를 가지고 있으며, 에코는 liver 와 비슷하거나 살짝 낮다. (따라서 liver 보다 밝고 크기도 1cm 미만으로 작으면 CKD 의심할 수 있다. 지방간이 있는 환자에게서 만성 신질환이 동반되어 있으면 정상처럼 보일 수 있으니 주의해야한다.)
Medulla 는 hypoechoic 하며, 사람에 따라 잘 보이는 경우도 있고, 뚜렷하게 잘 보이지 않는 경우도 있다. 양쪽을 비교해보면 되겠다. medulla 에 있는 pyramids 와 simple cyst 의 감별이 중요한데 simple cyst는 Anechoic, Well defined margin, Posterior acoustic enhancement 의 3가지 특징을 갖는다.
Renal sinus 는 fat tissue 가 있어 hyperechoic 하다. (Central echo complex 라고도 부른다.) 우리 신체 중에 가장 echogenicity가 높은 부위이기도 하다. 즉 renal sinus 와 echo 가 비슷한 liver 라면 Grade 3 이상의 fatty liver 임을 알수있다. 소아의 경우 fat이 적다. (놀라지 말 것.) 또한 renal siuns 부위에 ureter 가 늘어나있고, Hypoechoic 하게 보인다면 hydronephrosis 를 의심할 수 있다. hydronephrosis 가 생기면 renal pelvis 부터 늘어나기 때문에 hyperechoic 한 renal pelvis 에 tubular structure 가 있다면 hydronephrosis 가 생겼음을 알수 있다.
Renal artery
Main renal artery → Segmental a. (apical, upper, middle, lower, posterior) → interlobular a. (renal pyramids 사이) –> Arcuate artery (cortex 와 medulla 사이) –> Glomerular arteriole
RI 값은 interlobular a. 혹은 arcuate a. 에서 sampling 하여 측정할 수 있다. 이 중에 interlobular a. 의 경우 dopple 각이 60도 미만에서 만들어져 더 선호된다. RI 값은 parenchyma 로 갈수록 낮아져 0.7 미만이 정상값이 된다. (보통 0.6 정도가 정상)
* RI값이 높아지는 경우
- Renal a. stenosis (if measured upstream from the stenosis)
- Ureteric obstruction
- Extreme hypotension
- Very young children
- Perinephric fluid collection
- Medical renal disease
Doppler Resistance Index (RI) 계산기
Access sites for the kidneys
Rt. kidney 는 보통 liver 의 실질을 통과하여 비추면 잘 보인다. 반면 Lt. kidney 의 경우 위가 위치하여 잘 안보이므로 Rt. down decubitus 자세에서 posteriolateral 로 접근해야 잘 보인다. 거동이 힘들다면 좌측에 베게를 넣는 방법도 많이 사용된다.
*신장초음파 검사의 임상적 적응증
- 신장크기의 측정
- 요관막힘의 진단
- 신장종괴의 유무 및 감별진단
- 신장 실질의 해부학적 변화가 의심되는 경우신혈관을 평가하고자 할 때
Kidney 의 4 Questions
- 1. Size
- 2. Shape
- Regular renal profile or irregular renal profile
- 3. Parenchyma
- Cortical echogenecity
- Parenchymal thickness
- Cortisomedullary differentiation (소실될 경우 UTI 의심)
- 4. Hydronephrosis
Anatomical variants
1. Persistent fetal lobulation
- fusion 이 안되고 남아있는 모습. RCC 와 혼동이 가능하다.
2. Dromedary hump (단봉)
- Focal bulge on lateral border of Lt. kidney
- Result from adaptation of renal surface to adjacent spleen
- Easily differentiated from renal mass by doppler USG
- medulla 도 같이 튀어 나가기 때문에 내부에 medulla 음영을 볼 수 있으며, 도플러를 켜면 medulla 사이로의 interlobular a. 를 확인할 수 있다.
3. Prominent column of Bertin
- Cortical tissue indents the renal sinus
- RCC, TCC 와 감별이 필요하다.
- Continuity with renal cortex
- similar echo as renal parenchyma
- less than 3cm in size
- contains renal pyramids
- similar vascular pattern by color doppler
4. Parenchymal junctional defect
- commonly mistaken for cortical scar of angiomyolipoma
- (angiomyolipoma 의 경우 둥글고 뾰족하지 않다.)
- Triangular hyperechoic structure
- Continuity with central sinus by echogenic line ‘interrenicular septum’
5. Renal sinus lipomatosis
- Fat filled hypoechoic renal sinus mimicking mass lesion
- Absence of a well defined margin
- Normal vessels traversing renal sinus by CFD
Congenital anomalies of kidneys
1. Renal ectopia
- developmental renal anomaly characterised by abnormal anatomical location of one or both of the kidneys
- 초음파에서 한쪽 신장이 보이지 않는다면 다른 쪽 신장의 크기를 확인한다. 만약 크기가 정상이라면 Ectopic kidney 를 의심할 수 있겠고, 크기가 보상적으로 커져있다면 agenesis 를 의심할 수 있겠다.
2. Crossed fused ectopia
- Present when the kidney is seen in the opposite retroperitoneal space
- it is more common for the left kidney to be ectopically located on the right side.
3. Horsehoe kidney
- should be suspected when there is unable to detect lower poles of kidney
- RCC 빈도가 높고, Stone 이나 infection 의 빈도도 정상보다 조금 더 높다고 한다.
4. Ureteral duplication
- 2 central echogenic renal sinus with intervening bridging renal parenchyma
5. Ureterocoele
- Congenital dilatation of the distal-most portion of the ureter
- cystic structure projecting into the bladder (US finding)
6. Ureteropelvic junction obstruction
- Obstruction of the flow of urine from the renal pelvis to the proximal ureter
- UPJ obstruction is the most common pathologic cause of antenatally detected hydronephrosis
Pseudohydronephrosis
1. 신장의 혈류가 발달되어 있을 경우
2. Renal sinus cyst
- collecting system 과 연결되어 있지 않다.
- (1) Parapelvic cyst : 더 빈도가 많다.
- Hydronephrosis 라면 pelvis 가 먼저 늘어나야 하는데 그렇지 않다.
- (2) Peripelvic cyst : bilateral 한 경우가 잦다.
3. Extra renal pelvis
- Renal pelvis project outside the kidney medial to the renal sinus
- Refers to the presence of the renal pelvis outside the confines of the renal hilum
- Normal variation (-10% of the population)
- 소변을 채우고 비웠을 때 크기변화가 생긴다.
Boniak classification
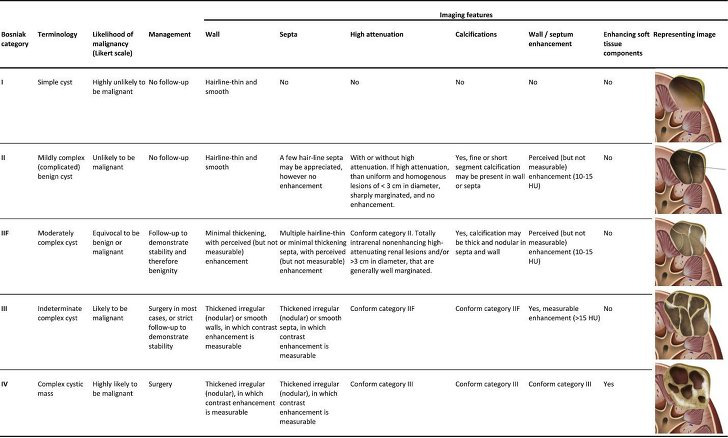
- I, II : f/u 불필요
- IIF : f/u 필요
- III, IV : 수술이나 시술 필요
Boniak I : simple cyst
- Simple cyst 의 3가지 US characteristics
- Anechoic
- Well defined margin
- Posterior acoustic enhancement
Boniak II : Minimally complex benign cyst
- Thin, well marginated
- Thin septa <1mm
- Thin calcification <1mm
- Hemorrhagic cyst
Boniak IIF : Indeterminate complex cyst
- 5년까지 f/u 하여야 한다. 6개월 → 1년 → 이후 매년 검사 (5년까지)
초음파에서 발견된 신종양의 접근법
- 정상변이 혹은 가성병변에 해당되는가?
- 낭성병변인가? 내부 성상은? Boniak classification
- Angiomyolipoma 같은 양성 종양의 특징을 가지는가? (수술 불필요)
- 악성종양을 시사하는 소견이 의심되어 조영증강 CT 등의 추가적인 영상검사 시행을 권고해야하는가?