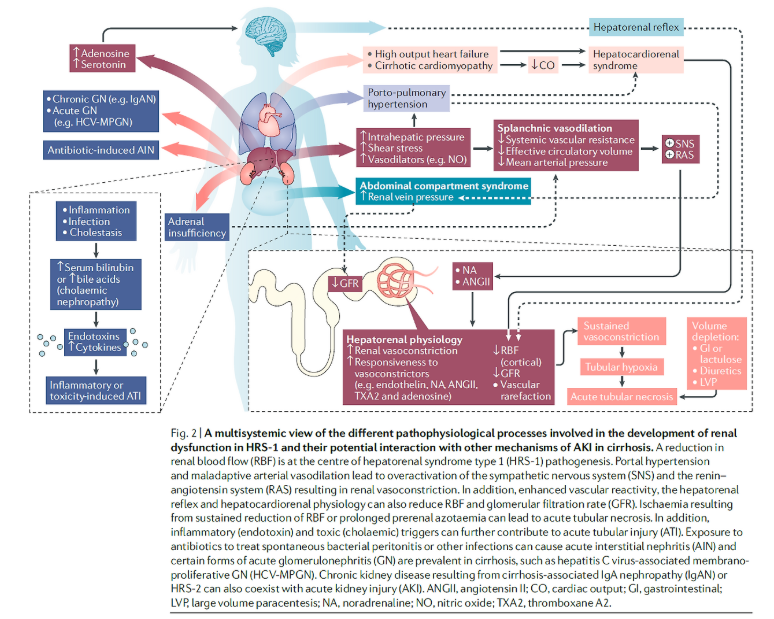
간경화는 만성 간질환의 진행된 형태이고 간 실질의 섬유화를 특징적으로 하는 상태입니다. 간경화가 있는 환자들은 급성신손상의 고위험군이기도 합니다. (간경화 입원 환자 중 급성 신손상의 발생율은 20% 정도라는 보고) 게다가 유효동맥혈량이 부족하며, 소화기나 소변으로의 수분 배설을 촉진하는 약들을 많이 사용합니다. 락툴로오스나 이뇨제가 그 예입니다. 또한 이러한 환자들은 신독성 항생제에 노출 되기 쉽습니다. 자발성 세균 복막염 등의 감염성 질환도 쉽게 발생가기 때문입니다. 그리고 대량 복수 천자를 할 경우에 혈역학적으로 불안정해질 위험이 존재합니다. 이러한 급성신손상의 기본적인 위험 요인도 있지만, 문맥 고혈압이 동반된 상당히 진행된 간경화에서는 특정한 형태의 급성신손상인 간신증후군 type 1 (= HRS-1) 이 발생할 수 있습니다. 간경화와 복수가 있는 환자의 경우 HRS-1 의 발생가능성이 5년내 40%까지 증가합니다. HRS-1 은 심각한 형태의 급성 신부전이며 사망률이 증가합니다. HRS-1 를 완벽히 치료할 수 있는 방법은 간이식입니다. 하지만 제한적일 수 밖에 없습니다. 따라서 HRS-1의 더 나은 진단과 치료를 위해서는 더 잘 이해해야 합니다.
HRS-1 의 예후가 대개 불량하지만, 적절한 시기에 치료하면, 혈관수축제 치료나 간이식으로 회복될 수 있습니다. 하지만 많은 환자들의 경우에는 신장애는 잘 회복되지 않습니다. HRS-1 의 기전은 혈역학적 인자들이 관여한다고 보고 있으나, 최근 연구에서는 비혈역학적인 인자들도 관여한다는 근거들이 제시되고 있습니다. 이러한 인자들을 서로 구분하여 진단하는 것은 어렵습니다. 따라서 종래의 HRS-1 의 진단 기준은 부족한 부분이 있습니다. 그러므로 각 급성신부전 환자들의 병태생리적 기전들을 이해하는 것이 적합한 진단과 치료전략 수립에 중요하겠습니다.
간경화 환자의 급성 신손상의 pathophysiology
몇가지 메커니즘이 간경화의 진행에 따라 급성 신손상의 발생에 기여합니다. susceptibility to kidney dysfunction 은 cirrhosis-induced circulatory dysfunction 과 maladaptive kidney perfusion 의 결합되어 발생합니다.
간질환이 진행될수록 circulatory and renal abnormalities 가 발생하는데, 이러한 현상을 hepatorenal physiology 라고 합니다. 동시에 간경화 환자들은 수많은 nephrotoxic elements (hypovolaemia, infections, bile acids and nephrotoxic medications) 에 노출 됩니다.
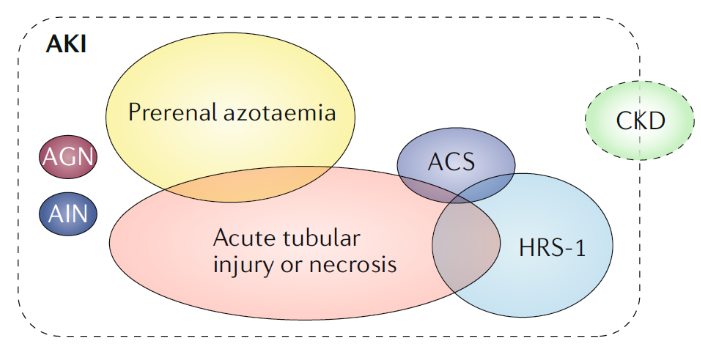
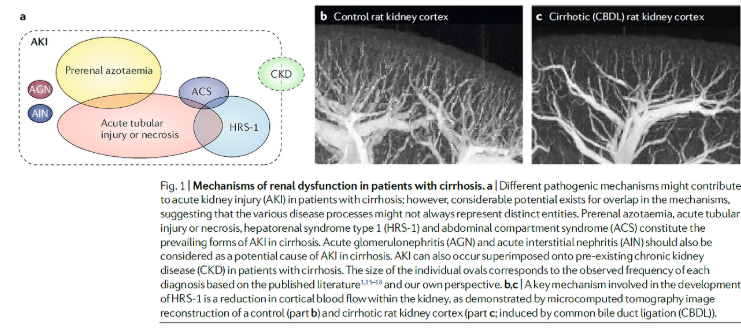
따라서 AKI 의 기본적인 원인인 prerenal azotaemia (PRA) 와 acute tubular necrosis (ATN) 또한 간경화 환자에서 발생할 수 있습니다. 간경화 환자에서 상대적인 PRA, ATN, HRS-1 or other causes of AKI 의 발생율은 각 연구마다 다양합니다. 전반적으로는 ATN (which affects ~15–60% of patients), PRA (affecting ~15–45% of patients) 이 HRS-1 (which affects ~10–40% of
patients) 보다는 좀 더 흔한 것 같습니다.
하지만 이제는 간경화 환자의 급성 신손상은 multifactorial etiology 를 가지고 있다는 것을 알고 있습니다. 따라서 순수한 HRS-1 환자는 오로지 hepatorenal physiology 의 결과로 신장애를 가지게 되는 일부 그룹일 뿐입니다.
1. Hemodynamic alterations in cirrhosis
HRS-1 에서의 신장애 기전은 궁극적으로 renal blood flow 를 저해하고 GFR 을 떨어뜨리는 circulatory derangement 와 관련이 있습니다. HRS-1 의 발생에 기여할 것으로 여겨지는 different haemodynamically-mediated pathophysiological processes 에 대해 살펴봅시다.
(1) Cirrhosis-induced circulatory dysfunction
간경화 환자들은 심한 그리고 진행되는 전신 혹은 국소적인 혈역학적 교란을 보입니다. 간실질의 구조가 계속 파괴됨으로써 이러한 derangements 는 촉발됩니다. 이로인해 intrahepatic vascular resistance 가 증가하여 문맥압이 증가하게 됩니다. 이로 인해 다양한 vasodilators 들이 local production 되어 splanchnic vasodilation (key component in the progression of circulatory dysfunction) 이 발생됩니다. 간이 더 나빠지거나 portosystemic shunting 으로 인해 과잉으로 생산된 vasodilators 은 Systemic vasodilation and a reduction in peripheral vascular resistance 를 일으킵니다. 이러한 mediator 들 중 nitric oxide 가 몇 가지 이유에서 흥미롭고 중요합니다. 첫번째는 mesenteric and renal vascular beds 를 포함하는 systemic and regional haemodynamics 에 중요한 regulator 이기 때문입니다. 두번째 이유는 increased sheer stress 에 반응하여 portal endothelium 에서 만들어지는 물질입니다. 세번째는 간경화 환자에서 haemodynamic derangements 를 충분히 발생시킬 수 있기 때문입니다. 마지막으로 간경화인 사람과 동물 모델에서 nitric oxide 의 level 이 증가해있고, nitric oxide production 을 저해하면 동물실험에서 cirrhosis-induced circulatory and renal impairment 를 완화하였습니다. HRS-1 을 예방하기 위해 정맥 알부민을 사용하는 것은 부분적으로 효과가 있을 수 있는데, 이는 nitric oxide level 을 낮출 수 있고, TNF 같은 cytokine 의 level 도 낮출 수 있기 때문입니다.
(2) Renal vasoconstriction
systemic vascular resistance 가 감소하고 nitric oxide-mediated splanchnic arterial vasodilation 되어 혈액이 pooling 되면 effective circulatory volume 의 감소를 유발합니다. 이러한 arterial underfilling 은 교감신경을 활성화 시키고, renin–angiotensin system (RAS) 을 항진시켜 effective circulatory volume 을 되돌려 놓으려고 노력합니다. 즉 noradrenaline and angiotensin II 이 분비되면 profound renal vasoconstriction and reductions in renal blood flow 를 유발하게 되면서 acute loss of GFR 을 일으키는 것입니다. 직접적인 관련성이 증명된 것은 아니지만, HRS-1 환자에서 plasma levels of noradrenaline, angiotensin II and renin activity 가 증가된 것을 보면 이러한 개념을 뒷받침하고 있습니다. 기저 간질환이 더욱 악화될수록 splanchnic and systemic arterial vasodilation 는 compensatory capacity 를 벗어나게되고 mean arterial pressure 의 감소를 초래합니다. 이는 tissue and organ perfusion 을 저해할 수 있습니다.
(3) Derangements in renal microcirculation
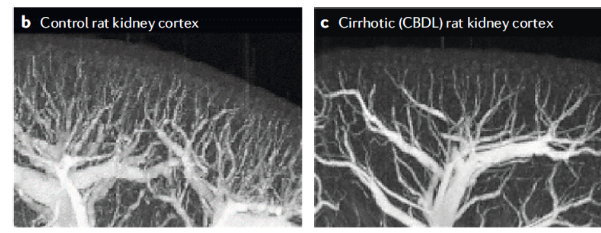
medullary blood flow 가 먼저 감소되는 일반적인 ischimic AKI 와는 다르게 HRS-1 에서 발생하는 renal blood flow 의 저하는 우선적으로 cortical blood flow 의 저하와 관련이 있습니다. Use of microcomputed tomography has demonstrated that chronic bile duct ligation to induce liver fibrosis in rats induces a decrease in renal perfusion characterized by decreased vascular filling of the renal cortex. 이러한 vascular volume 의 저하는 profound, refractory regional vasoconstriction 으로 인해 발생되었습니다. 그러나 상당히 진행된 간경화에서는 vascular rarefaction 도 관여하는것으로 여겨집니다. 따라서 간경화 환자에서 지속되는 교감신경계와 RAS 의 활성화는 hypoperfusion 을 지속시키고, 이는 ischemic insult 를 조장하여 renal microvascular endothelial injury, vascular rarefaction and other irreversible defects in the kidney cortex 를 촉진시킵니다.
(4) Vascular reactivity
Vascular reactivity 는 responsiveness of a blood vessel to a specific stimulus or compound 를 의미합니다. 간경화 동물 모델에서 renal vascular reactivity 가 항진되어 있다는 것을 확인하였습니다. 예를 들면 renal arterioles of rat models 은 bradykinin 에 vasodilatory response 가 저하되어 있는 것을 보여주었고, augmented contractile response to noradrenaline, endothelin 1, angiotensin II 을 보여주었습니다. 이러한 메커니즘에는 Endotoxaemia and reactive oxygen species 이 관여할 것이라고 추정하고 있습니다.
임상적으로 보이는 것과 같이 HRS-1 에서 특징적인 renal haemodynamic alterations 은 결국 치료를 더욱 어렵게 하며, 지속적인 신장애를 일으키는 메커니즘이 존재하는 것 같습니다.
이러한 치료 저항에 대한 설득력있는 설명은 지속적인 renal cortical hypoperfusion and rarefaction 인데, renal vascular hyperresponsiveness 와 함께 신기능 장애를 악화시킨다는 것입니다. ischaemic insult and intrinsic tubular injury 와 유사하며, 이는 결국 irreversible kidney damage and dysfunction 을 일으킵니다.
(5) The hepatorenal reflex
실험적 근거들이 간에서 시작되어 renal sympathetic nerve activity 의 변화를 야기하는 hepatorenal baroreflex 의 존재를 지지합니다. hepatic sinusoidal pressure 의 변화는 local release of adenosine 을 촉진하고 이는 hepatic afferent SNS (sympathetic nerve system) 을 활성화 시켜 brain 과 efferent renal SNS 를 통해 신장으로 신호가 건너가서 renal vasoconstriction 을 일으킵니다. hepatic afferent SNS 의 활성화에 serotonin 이 neurotransmitter 로 주목받은 적이 있습니다.
Portal vein 을 막아 문맥압을 증가시켰더니 immediate reduction in renal blood flow 가 발생하였고, 카테터를 deflation 시켜 문맥압을 정상화 시켰더니 즉시 renal blood flow 가 회복되었다는 연구가 있습니다. 이러한 현상은 MAP 나 effective circulatory volume 감소 없이도 발생하였고, 이는 HRS-1 에서 보이는 systemic neuro-humoral activation 과는 독립적인 liver–kidney crosstalk 의 존재를 생각해볼 수 있겠습니다.
이 가설을 지지하는 또 다른 증거는 다음과 같은 것들이 있습니다.
– Hepatic denervation led to a reduction in renal sympathetic nerve activity in a rat model of cirrhosis
– Whereas lumbar sympathetic block led to improvement in kidney function in five patients with chirrosis with estimated GFR <25 ml/min
따라서 hepatorenal reflex 는 cirrhosis-induced renal dysfunction 이 있는 환자들에게 potential therapeutic implications 이 있는 불가사의한 메커니즘으로 남아있습니다.
(6) Cirrhotic cardiomyopathy
간경화 환자에서 Circulatory homeostasis 는 hyperdynamic circulation 으로 인해 유지됩니다. 여기에는 increased cardiac output, heart rate and plasma volume 이 포함됩니다. 간경화가 더욱 진행하면, state of high cardiac output 에서 one of cardiac dysfunction 으로 변하게 됩니다. 여기에는 blunted cardiac responsiveness, impaired diastolic relaxation, electrophysiological conductance abnormalities with chronotropic ncompetence and decreased cardiac output 등의 특성이 있습니다. 이러한 장애를 cirrhotic cardiomyopathy 라고 합니다. cirrhotic cardiomyopathy 이 circulatory dysfunction 에 미치는 영향은 low cardiac output with decreased renal blood flow, decreased GFR 과 a higher probability of developing HRS-1 의 관련성에 의해 support 됩니다.
어떤 연구에서는 decreased cardiac output in the setting of HRS-1 를 보고하였습니다. beta-blockers 를 사용하는 등의 haemodynamic stress 에서 Systolic dysfunction이 발생할 수 있습니다. 실제로 비보상성 간경화 환자에서 non-selective beta-blockers 를 사용하는 것은 HRS-1 의 발생을 높일 수 있습니다. 진행된 간경화 환자에서 나타날 수 있는 Autonomic dysfunction and reduced baroreflex sensitivity 또한 altered haemodynamics and the reduction in cardiac output 을 유발할 수 있습니다. 간경화 환자에서 cardiac dysfunction 과 kidney dysfunction 과의 연관성은 transjugular intrahepatic portosystemic shunt (TIPS) 를 통해 알수도 있습니다. TIPS 를 거치하면 considerable displacement of blood to the central vascular compartment 이 발생하여 marked increase in preload, stroke volume and kidney function 을 일으킵니다. 따라서 간경화 환자에서 심기능의 다양한 이상을 보이는 경우 careful examination of cardiorenal involvement 이 필요하겠습니다. 이러한 측면에서 ‘hepatocardiorenal’ syndrome 이라는 용어가 제안되기도 했습니다. — describe the interaction between the kidney, liver and heart in the context of cirrhosis
(7) Porto-pulmonary hypertension
간경화와 문맥고혈압이 있는 환자는 폐고혈압의 위험이 증가합니다. 어떤 연구에서는 그 발생율을 5~10% 정도로 보고한 바 있습니다. 이러한 견지에서 porto-pulmonary hypertension (PoPH) 이라는 용어가 나왔고, 간이식의 적합성을 평가할때 사용되기도 합니다. porto-pulmonary hypertension 의 기전은 lung vascular smooth muscle cell hypertrophy, in situ thrombosis, vasoconstriction and the development of venovenous shunts, triggered by factors such as serotonin, IL-1, endothelin 1 and thromboxanes 을 포함합니다. porto-pulmonary hypertension 이 further compromises the circulatory derangements of HRS-1 를 유발할 수 있겠지만, porto-pulmonary hypertension 자체가 직접적으로 renal
impairment in HRS-1 에 기여하는지는 아직 확실치 않습니다.
(8) Intra-abdominal hypertension
Paracentesis-induced circulatory dysfunction (PICD) 는 대량 복수천자 이 후 일시적으로 plasma renin activity 가 상승하는 것이 특징입니다. HRS-1 환자에 대한 초기 연구에서
대량 복수천자가 신기능 장애에 선행했다는 것을 알아냈습니다. 그러나 대량복수천자가 HRS-1 의 선행 원인이라는 근거는 아직 확립된 바가 없습니다. PICD 에 대한 연구 대상자는 우선적으로 정상 신기능 혹은 안정적인 만성신부전 환자 (AKI 환자가 아닌) 를 대상으로 진행되었습니다. 게다가 IV albumin 을 예방적으로 사용하는 경우가 증가하면서 간경화 환자의 PICD 의 발생율은 거의 절반으로 감소되었습니다. (albumin 은 복수를 제거하는 동안 적절한 arterial blood volume 을 유지하는 수단이 됩니다.) 그러나 tense ascites 를 가진 증가된 IAP (intra-abdominal pressure) 의 경우 IAH (intra-abdominal hypertension), Abdominal compartment syndrome 을 유발할 수 있고, renal vein 의 pressure 를 증가시켜 신기능의 감소를 일으킬 수 있습니다. 따라서 간경화 환자에서 대량 복수천자를 통해 복압을 완화시키는 것은 일시적인 GFR 의 증가와 소변량 증가를 유도하였다는 보고도 있습니다. 게다가 치료적 대량 복수천자 이 후 AKI 가 호전된 케이스들이 나타나기도 했습니다. 그럼에도 불구하고 IAP 의 systemic surveillance 와 reactive LVP 가 HRS-1 의 환자의 임상 경과를 좋게 만들 수 있는지는 아직 밝혀지지 않았습니다.
(9) Adrenal insufficiency
비대상성 간경화와 복수를 가진 환자에서 Adrenal insufficiency 는 25–65% 정도로 보고 되는데, ‘hepatoadrenal syndrome’ 이라고도 불립니다. hepatoadrenal syndrome 의 유병률은 간질환의 중증도가 심할 수록, 급성 질환이 동반될 수록 증가하는 것처럼 보입니다. Adrenal insufficiency 는 간경화와 급성신손상이 동반된 환자에서 potentially further compromise circulatory function 과 reduce systemic blood pressure 를 유발할 수 있습니다. 한 연구에서는 간경화와 HRS-1 인 환자들이 HRS-1 이 없는 환자들에 비해서 adrenal insufficiency 발생율이 더 높은 것을 보고 하였습니다. 이 연구에서는 또한 baseline adrenal insufficiency 와 risk of subsequently developing HRS-1 의 연관성에 대해서도 보고하였습니다. 하지만 HRS-1 환자에서 adrenal insufficiency 가 kidney haemodynamics 와 임상적 경과 및 vasoconstrictor therapy 의 반응에 영향을 미치는지는 아직 분명치 않습니다.
2. Non-haemodynamic derangements
간경화 환자에서 신장애를 일으키거나 악화시킬 수 있는 다른 인자들도 있습니다.
(1) Progression to acute tubular injury or necrosis
HRS-1 가 지속되면 결국 tubular insult 로 진행된다는 보고가 있습니다. 비록 간경화 AKI 환자에서 신장조직검사는 거의 시행되지 않으나, HRS-1 환자의 경우 신장 실질의 morphological changes 는 상대적으로 minimal 했다는 보고도 있습니다. 실제로 HRS-1 환자의 신장 조직 (부검)에 대해 전자현미경으로 분석해보면 tubulorrhexis and the presence of dark bodies in mitochondria — indicative of ATN 을 확인할 수 있섰습니다. 게다가 HRS-1 환자의 부검 조직에서 distinctive lesion involving reflux of proximal convoluted tubule epithelium into the Bowman space 이 확인되기도 하였습니다.
이식에 관련된 연구에서 또한 HRS-1 환자에서의 progressive kidney injury 가 있다는 사실을 지지하고 있습니다. 이식 센터에서 대부분 사용하는 표준 프로토콜은 투석을 시작하는 HRS-1 환자에서 4~6주내에 donor liver 가 준비되는 경우 간 이식 단독을 권유한고, 투석을 한지 6주 이상이 지난 환자의 경우 liver-kiney를 같이 이식하는 것이 권유됩니다.
이러한 접근은 HRS-1 의 간 이식 후 회복 정도는 이식 전 투석을 유지한 기간에 반비례 하는 연구결과에 기인합니다. 이런 결과에 대한 논리적인 설명은 간경화 환자에서 sustained AKI 와 renal vasoconstriction 은 결국 ischaemic insult and intrinsic tubular injury 로 변화한다는 것으로 설명할 수 있습니다. vasoconstrictor therapy 에 대한 HRS-1 치료 반응은 serum bilirubin 이 높을수록 감소하는데, 이는 serum bilirubin 이 높을수록 cholaemic nephropathy 와 비슷한 기전으로 AKI를 악화시키기 때문일 것입니다. 이러한 내용은 association between the severity of hyperbilirubinaemia and the likelihood of detecting renal tubular epithelial cell casts — 이것은 ATN 의 marker 이다. — 을 보고한 2019년 연구부터 support 되어 왔습니다. 간경화에 대한 동물 연구에서는 intrinsic tubular injury 가 time-dependent development 한다는 것을 보였다. 이러한 발견은 HRS-1 의 발생기전이 purely functional renal impairment 에서부터 overt tubular damage 로 변화해 가는 스펙트럼으로 보는 것이 알맞을 것입니다.
그러나 temporal progression of HRS-1 의 근거는 아직 부족한 실정입니다.
(2) Bile acids and cholaemic nephropathy
Cholaemic nephrosis 는 옛날 용어인데, 현재는 cholaemic nephropathy 로 용어가 바뀌었습니다. 이는 “patients who acquire AKI in the context of obstructive jaundice” 를 의미합니다. 이러한 상태는 담낭암이나 다른 담도의 기계적 폐쇄가 있는 상태의 환자들에게서 나타났으며, 동시에 acute tubular injury (ATI) and peritubular venular dilatation 가 발생합니다. 흥미로운 점은 infections or drugs, such as anabolic steroids 로 인한 cholestasis 의 경우 AKI 가 나타날 때, 조직검사상 tubular injury with bile cast deposition in the tubular lumen 가 보인다는 점입니다. 이를 bile cast nephropathy 라고 합니다. 부검 연구에서는 간경화 환자이고 serum bilirubin 이 매우 상승한 환자의 경우 조직검사상 tubular injury with intraluminal bile casts 가 보였다는 연구결과가 있습니다. 이러한 소견은 원인을 알아내기 어렵기 때문에 그 결과의 해석에 주의해야 합니다. 의문은, presence of intratubular bile casts 만이 오로지 decreased GFR and tubular
stasis or a cause of tubular injury 를 반영하는가 입니다. 수년전 한 연구에서는 bilirubin-stained renal tubular epithelial cell casts 이 황달이 심한 간질환 환자에서 주로 보이고, 황달이 없는 간질환 환자에서는 보이지 않는다는 결과가 있는데, 이는 association between severe hyperbilirubinaemia and tubular injury 를 지지해줍니다. 역설적이게도 bilirubin 은 renoprotective 한 속성이 있다고 알려져 있습니다. 따라서 bilirubin cast nephropathy 라는 말이 좀 이상할 수 있습니다. 하지만 bile acids can elicit tubular damage, tubulointerstitial inflammation, and lipid peroxidation and oxidative stress in the kidney. 따라서 cholaemic nephropathy 라는 일반적 용어가 제시되었습니다.
AKI 상태에서 bilirubin excretion 의 변화는 무시할 수 없습니다. 따라서 cholestasis 로 인한 Serum bilirubin 의 상승은 AKI 단독으로도 더욱 심해질 수 있습니다. 이러한 결과는 hyperbilirubinemia 가 있는 환자에서 AKI 의 평가를 더욱 복잡하게 합니다. hepatorenal physiology 에서의 functional changes 와 cholaemic nephropathy 와의 구별을 더욱 어렵게하기 때문입니다. 현재 cholaemic nephropathy 가 deranged renal haemodynamics of HRS-1 에 superimposed 될 수 있다는 근거는 없습니다. 더 많은 연구가 필요하겠습니다.
(3) Inflammation
진행된 간경화에서 증가된 serum levels of pro-inflammatory cytokines (endotoxins, interleukins and TNF) 가 연관이 있었습니다. 이러한 cytokine 들은 SBP or acute-on-chronic liver failure (ACLF) 환자들에서도 증가되어 보이는데, 이들은 common triggers of HRS-1 입니다. 간경화 또는 cholestasis 의 상황에서 발생하는 inflammation 은 아마도 장에서 혈류로 Bacteria 의 translocation 으로 인해 endotoxin 이 분비되어 유발되는 것으로 추정됩니다. 간경화 AKI 환자의 신장조직검사에서 renal tubule 에 endotoxin receptor, Toll-like receptor 4 (TLR4) 의 overexpression 이 확인된다는 보고가 있습니다. Pro-inflammatory cytokines 은 endothelial dysfunction and tubular injury 를 유발할 수 있습니다. Pathogenesis of AKI in cirrhosis may involve both haemodynamic changes typical of HRS-1 and inflammation-induced ATI