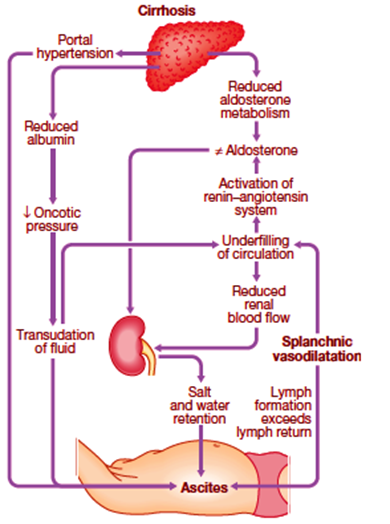
Ascites 의 pathophysiology
– 문맥압 상승
–> 국소 혈관 확장 물질 생성 증가 (주로 NO)
–> Splanchnic arterial vasodilatation
–> Effective arterial blood volume 의 저하
–> 교감신경계, RAAS 항진, ADH 증가
–> 신장에서의 Na 저류, 세포외액 증가
–> 복수, 부종, Hyponatremia 발생.
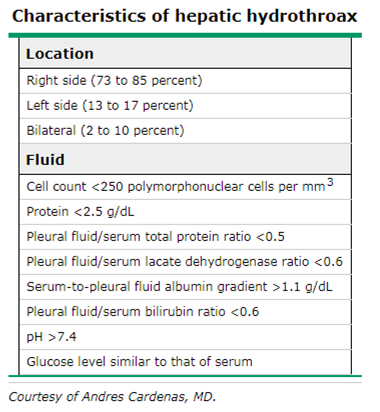
Hepatic hydrothorax 란?
Presence of a pleural effusion in a patient with cirrhosis
– does not have other reasons to have a pleural effusion (eg, cardiac, pulmonary, or pleural disease)
– usually > 500 mL
– occurs in approximately 5 ~ 10 % of LC

Hepatic hydrothorax 의 pathophysiology
Small diaphragmatic defects
–> Probably results from the passage of ascites
left hemidiaphragm is thicker and more muscular (Rt > Lt side)
Negative intrathoracic pressure
– Promotes the passage of fluid
– some patients with hepatic hydrothorax do not have apparent ascites.
Treatments of Ascites
(hepatic hydrothorax 의 기본치료와도 비슷하다.)
기저 간질환의 치료
– 금주, 항바이러스제
비약물적 복수 치료
– 염분섭취제한
–> 하루 염분섭취량 5g = Na 2g = 88 mEq
– 수분섭취제한
약물치료 – 경구 이뇨제
– Aldosterone antagonist (기본적인 이뇨제)
–> Spironolactone : 하루 50~100mg 으로 시작, 최대 400mg
(Amiloride – 항안드로겐 작용 적음, spironolactone의 1/10 용량으로 사용)
– Loop diuretics
–> Furosemide : 하루 20~40mg 로 시작 최대 160mg
(Torsemide – 반감기와 작용 시간이 김. furosemide의 1/4 용량으로 사용)
– 추천 비율은 100:40
이뇨제의 치료 반응 평가
체중감소
- 부종이 있는 경우 하루 약 1kg 이내
- 부종이 없는 경우 하루 0.5kg 이내
- 염분섭취제한 (하루 염분섭취량 5g – Na 2g, 88 mEq)
- 소변외로 배출되는 Na 10 mEg –> 나머지 78 mEq 이 소변으로 배출
- Spot urine Na/K ratio 1이상이면 24시간 소변 Na 78 mEq 이상일 확률 90~95%
- 체중감량이 충분하지 않은 환자
- 24시간 소변 Na 가 78 mEq 이상 : 염분섭취제한이 안되고 있음.
- 24시간 소변 Na 가 78 mEq 미만 : 이뇨제 효과가 충분하지 않음 -> 이뇨제 증량
Hepatic Hydrothorax 의 치료
Persistent hydrothorax despite a sodium-restricted diet and diuretic therapy
– Repeated thoracenteses
– TIPS placement
– Pleurodesis
– Surgical repair of defects in the diaphragm
– Liver transplantation
Repeated thoracenteses
The most effective way to reduce large effusions (greater than 1.5 L)
기존의 2L 법칙 – 폐부종, 저혈압 방지 위한 – 보다 더 뽑는 것이 가능할 것임.
Chest tubes should not be placed
– 이유 ? massive protein and electrolyte depletion, infection, renal failure, and bleeding
– may be needed for patients with spontaneous bacterial empyema and frank pus, or in patients undergoing pleurodesis
Pleurodesis
2주~3주에 한 번꼴로 자주 Thoracentesis 가 필요할 경우
Chemical pleurodesis is commonly used
– most difficult form of nonmalignant pleural effusion to treat with chemical pleurodesis
– rapid migration of fluid from the abdomen into the pleural space
– often difficult to keep the two pleural surfaces apposed long enough for the inflammatory process
난치성 복수 (refractoray ascites)
염분섭취제한과 최대용량의 이뇨제에도 불구하고 조절되지 않거나 복수천자 후에도 배로 재발하는 경우
이뇨제 저항성 / 이뇨제 불응성
Pre-hepatorenal syndrome
Poor prognosis (6M survival 50%, 1Y survival 25%)
난치성 복수의 Initial Treatment
Stop medications
–> that decrease systemic BP (renal perfusion)
– ACEi, ARBs
– Beta blockers
– NSAIDs (<– Renal vasoconstriction)
Oral midodrine
Continuation of sodium restriction
Diurectics
– 언제 중단해야하는가?
– Continued only when UNa excretion > 30 mEq/day
(이뇨제로 인한 합병증 발생시, UNa 30 미만이면 중단)
Discontinuing beta blockers
Potential to reduce renal perfusion
Leading to decreased natriuresis
Some studies suggest a/w increased mortality rates.
– May occur because failure to maintain an adequate MAP
Oral midodrine
– Vasopressor –> BP 상승 –> renal perfusion 향상 –> Renal Na excretion 향상
– Start 5mg tid –> 2.5mg 씩 증량 (최대 17.5mg tid) MAP > 82 mmHg 목표
Options if initial Treatments fail
Liver transplantation
Serial therapeutic paracenteses
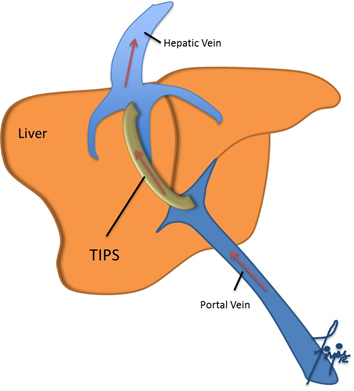
TIPS (Transjugular intrahepatic portosystemic shunt) placement
Large-volume paracenteses
– Mainstays in the treatment
– 단백질 소실, 감염위험 증가, Post-paracentesis circulatory dysfunction
– 복수 5L 이상의 대량 천자시 1L 당 albumin 8~10g 주입 권장, Midodrine, terlipressin 사용 가능.
TIPS placement
Complication
– Hepatic encephalopathy (30% of patients)
– Early thrombosis or delayed shunt stenosis
– (22~50% of uncoated stents –> 이제는 Gore-Tex covered stents 사용)
Not good candidates for TIPS
– Child-Pugh class C (>12), high MELD score (>18)
– Heart failure
– Severe spontaneous hepatic encephalopathy
Other invasive treatments
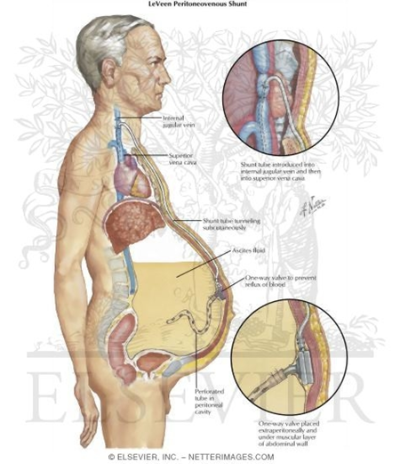
Peritoneovenous shunt (LeVeen or Denver shunt)
: Ascitec fluid –> IJV
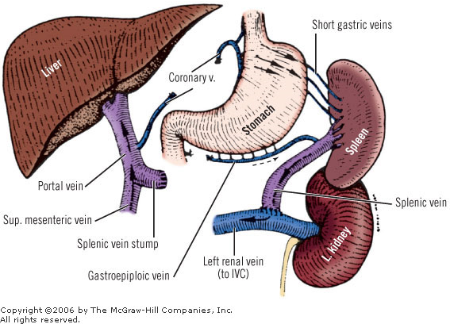
Surgical portasystemic shunts (e.g. Distal splenorenal shunt)
Experimental Treatments
Vasopressin receptor antagonists
Splenic artery embolization
Hypertonic saline plus a loop diuretics
Clonidine
– Alpha-2 adrenergic receptor agonist)
–> suppressed RAAS
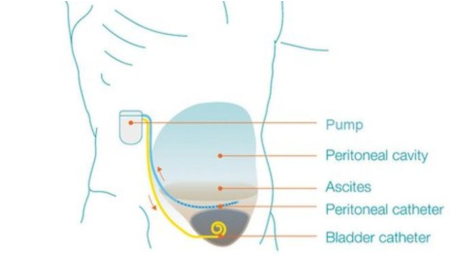
Low-flow ascites pump
Low-flow ascites pump