여성형 유방의 기전
남성 유방조직은 에스트로겐과 안드로겐의 protein receptor 를 가지고 있다.
에스트로겐은 mammary ductules 를 proliferation 시키고
안드로겐은 이 작용을 억제한다.
이러한 호르몬의 불균형이 여성형 유방을 만드는 주된 기전이다.
estrogen/androgen 불균형 원인 : estrogen 이 증가할 때
(1) 고환이나 부신에서 분비되는 free estrogen level 이 증가
(2) extraglandular aromatization of estrogen precursors
(3) decreased estrogen degradation
(4) exposure to estrogen-like chemicals or exogenous estrogens
(5) use of drugs that cause displacement of more estrogen than androgen from sex hormone-binding globulin (SHBG)
estrogen/androgen 불균형 원인 : androgen 이 감소할 때
(1) decreased androgen production in the testes
(2) increased binding of androgens (relative to estrogens) by SHBG
(3) altered androgen metabolism
(4) drug-induced displacement of androgens from their receptors
(5) androgen receptor defects
남성은 testes 에서 circulating testosterone 95% 를 분비 (estradiol 15%, estrone 5%) 한다.
정상 남성에서 estrogen 의 혈중 농도는 매우 낮다. 대부분의 estrogen 은 (80%) two precursors (androstenedione, testosterone)에 의한 peripheral conversion 으로 생성되는데 각각 estrone, estradiol 이다. (aromatase 가 작용한다.) Peripheral conversion 은 intramammary 와 subcutaneous fat 에서 주로 발생하나 liver, skin, muscles, kidneys 에서도 일어난다. Aromatase activity 는 나이가 많아질수록, BMI가 증가할 수록 커진다.
대부분의 여성형 유방을 가진 남자 환자들은 serum prolactin levels 이 높지는 않다.
또한 hyperprolactinemia 라고 해서 전부 여성형 유방이 생기는 것도 아니다.
여성형 유방의 원인
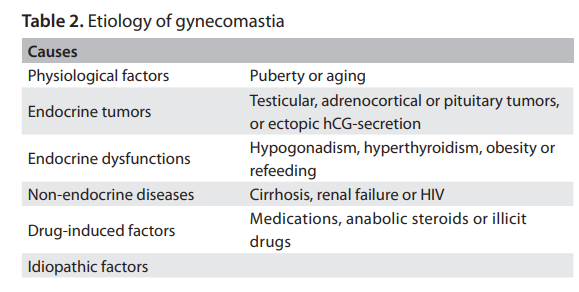
Pubertal Gynecomastia
사춘기 GM은 대체로 13~14세 무렵에 경미한 정도로 나타나며, 6~12개월간 지속되다가 95%에서 자연적으로 소실된다. Glandular enlargement는 비대칭적일 수 있고 압통이 동반될 수 있다.
병태생리학적으로는 androgens에 비해 estrogens의 혈청 농도가 상대적으로 과잉되는 것이 관여하는데, 이는 estradiol 생성이 testosterone 생성보다 먼저 증가하기 때문이다.
Aging Gynecomastia
65세 이상의 고령 남성에서는 흔히 상대적 hypogonadism이 나타나며, 이는 plasma testosterone 수치의 감소, SHBG 상승, free testosterone 감소로 특징지어진다. 또한 진행성 비만으로 인해 말초 aromatase activity가 증가한다. 이 연령대에서는 여러 동반질환이 흔하며, 복용하는 약제 역시 gynecomastia를 유발하거나 악화시키는 데 기여할 수 있다.
Endocrine tumors
(1) Benign testicular tumors (Sertoli or Leydig cell tumors)
Benign testicular tumors (Sertoli 또는 Leydig cell tumors)는 estradiol을 분비할 수 있다. 이로 인해 LH 수치가 2차적으로 억제되어 testosterone 합성에 부정적인 영향을 미친다. 상승된 estrogen 수치는 혈청 SHBG 농도를 증가시키며, SHBG는 testosterone에 선호적으로 결합하여 free testosterone 수치를 낮춘다.
(2) Choriocarcinoma and other germ cell tumors
Choriocarcinoma 및 기타 germ cell tumors는 hCG를 생성하여 고환의 Leydig 세포를 자극해 estradiol 분비를 촉진하고, 종종 GM을 유발한다. 이러한 종양은 촉진 시 만져질 수도 있고, 초음파를 통해서만 발견될 수도 있다. 또한 폐, 간, 위, 신장 등에서 기원한 ectopic hCG 분비 종양 역시 GM을 일으킬 수 있다.
(3) Pituitary adenomas
Prolactin을 분비하는 pituitary adenomas (prolactinomas) 역시 GM을 유발할 수 있다.
(4) Adrenocortical tumors
Adrenocortical tumors는 일반적으로 젊거나 중년 남성에서 흔히 발생하는 큰 악성 종양이다. 이들은 estradiol 및 androstenedione 같은 steroid 전구체를 직접 분비하는 feminizing tumors이다. 혈청 estrogen 상승은 또한 LH 매개 testosterone 생성을 억제한다.
Endocrine dysfunctions
(1) Severe hyperthyroidism
Severe hyperthyroidism increases serum SHBG. Since estradiol
binds less avidly to SHBG than does testosterone, there appears to
be an increase in the ratio of free estradiol to free testosterone, thus
resulting in clinically evident GM in 10 to 40% of the patients.
(2) Primary gonadal failure
– testicular trauma, chemotherapy, mumps, orchitis, leprosy
– Klinefelter syndrome
– Male pseudohermaphroditism with Morris syndrome
– long-standing type 1 diabetes (diabetic mastopathy)
– metabolic syndrome
– refeeding after severe starvation
– substantial weight loss
– functional hyperprolactinemia
Primary gonadal failure는 testicular trauma, chemotherapy, mumps, orchitis, leprosy로 인해 발생할 수 있으며, 이는 혈청 testosterone 수치를 낮추어 LH 상승을 유발하고, 남아 있는 Leydig 세포를 자극하여 estrogens 분비를 촉진함으로써 GM을 일으킬 수 있다.
Klinefelter syndrome은 염색체 이상(47, XXY karyotype)으로, hypogonadism과 불임과 연관된다. 이러한 남성의 약 70%에서 GM이 관찰된다. 추가 X 염색체의 존재가 GM과 연관되는 이유는 명확하지 않다.
Male pseudohermaphroditism인 Morris syndrome (testicular feminization)은 gonadal estrogen 생성으로 인해 정상 여성의 유방과 유사한 형태가 동반되는 경우가 많다. 이때 낮은 testosterone과 상승된 LH는 primary hypogonadism을 시사한다. 반면, 낮은 testosterone 수치와 정상 LH 수치는 secondary testicular failure를 나타낸다.
장기간의 제1형 당뇨병을 가진 남성에서 diabetic mastopathy가 발생할 수 있는데, 이는 한쪽 또는 양쪽 유방의 단단하고 광범위한 종대로 나타난다.
이 외에 GM 발생과 관련된 endocrine-metabolic condition으로는 metabolic syndrome, 심한 기아 후의 refeeding, 상당한 체중 감소, functional hyperprolactinemia 등이 있다.
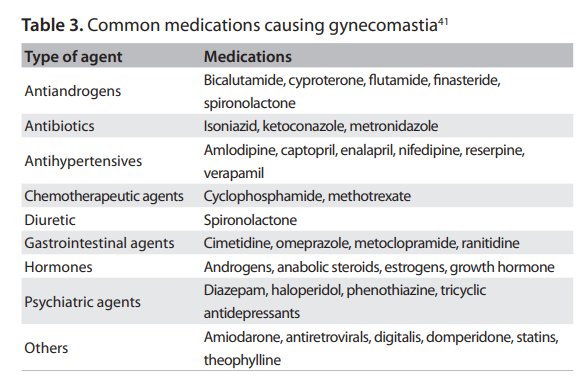
약물로 인한 여성형 유방
여성형 유방(GM)과 가장 흔히 연관되는 약물 중 하나는 이뇨제인 spironolactone으로, 이는 aldosterone에 대한 경쟁적 길항제이다. Spironolactone은 또한 고환에서 testosterone 생성을 억제하고, testosterone의 estradiol로의 aromatization을 촉진하며, 일부 조직의 androgen receptor에 결합하여 항안드로겐(antiandrogenic) 효과를 나타낸다.
Prostate cancer에 대한 androgen deprivation therapy에서도 흔히 부작용으로 GM이 나타난다. GM의 발생률은 호르몬 치료의 종류와 기간에 따라 다르지만, 최대 40~70%에 이를 수 있다.
Cocaine, heroin, amphetamines와 같은 불법 약물 및 기타 남용 약물 역시 GM과 흔히 연관된다. Marijuana는 estrogen receptor에 작용하며 phytoestrogen으로 작용하는 것으로 알려져 있다.
또한 anabolic androgenic steroids, gonadotropins, growth hormones를 이용한 도핑은 파워 스포츠 및 웨이트 트레이닝에서 광범위하게 이루어지고 있다. 남성 운동선수에서 이러한 의인성 약물(iatrogenic drugs)은 spermatogenesis 억제 및/또는 GM 유발을 초래할 수 있다.
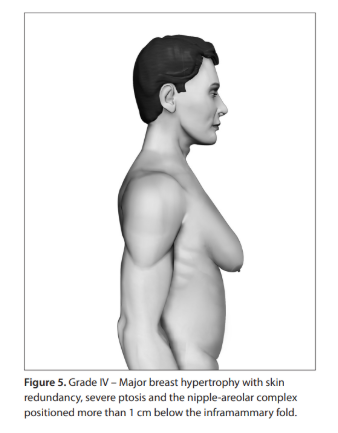
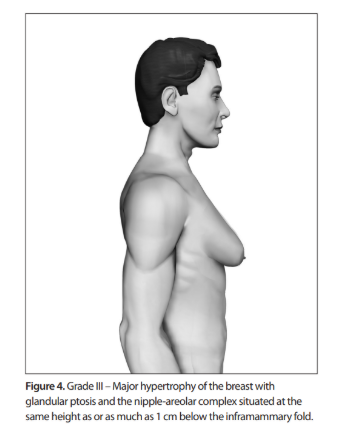
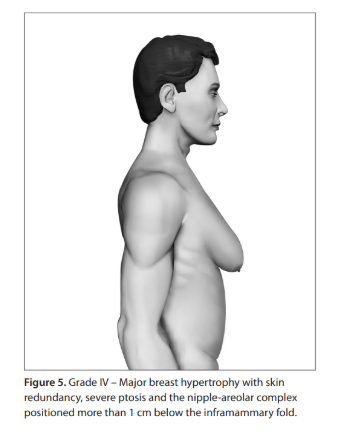
여성형 유방의 중증도 분류
참고문헌 : Sao Paulo Med J. 2012; 130(3):187-97