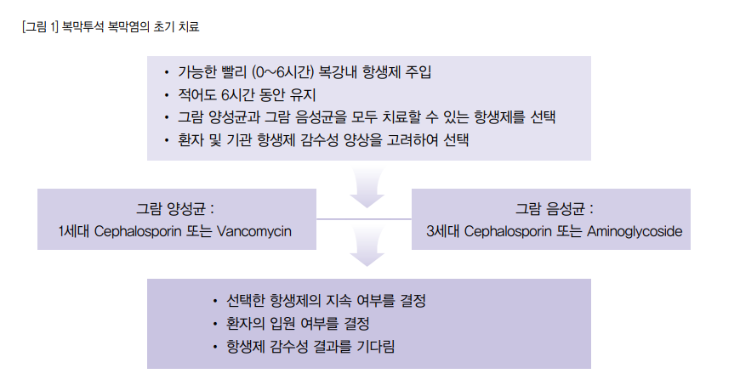
Exit site infection
가장 흔한 원인균은 S. aureus 이며 비교적 흔하면서도 심각한 균은 P. aeruginosa 이다. 치료는 1세대 세팔로스포린이나 Penicillase-resistant penicillin 를 S. aureus 를 cover 하기 위해 empirical oral antibiotics 로 선택한다. 다만 이전 MRSA 나 Pseudomonas spp. 의 감염 혹은 colonization 되지 않았었던 환자여야 한다.
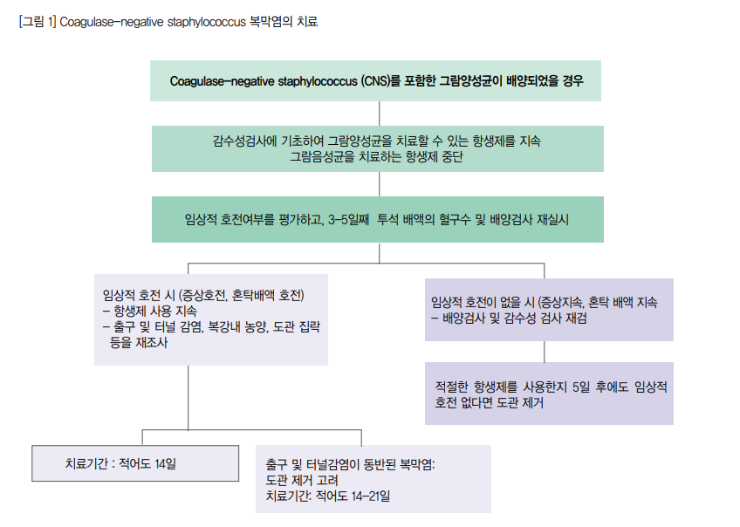
(1) Gram positive 균이라면 S. aureus 를 생각하고, 1세대 세팔로스포린이나 Penicillase-resistant penicillin 을 사용하며, 만일 MRSA 의 감염 병력이 있다면 IP Vancomycin 을 사용할 수 있다. 그럼에도 5~6일까지 사용해보았는데도 반응이 없다면 Rifampin 을 추가해 볼 수 있다. (Gram positive 라면 보통 2주 이상 치료한다.)
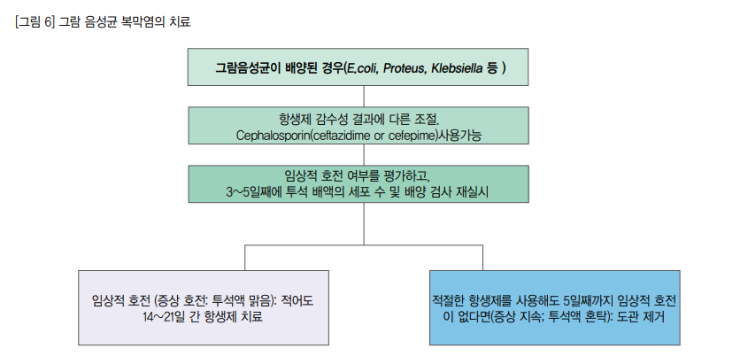
(2) Gram negative 균이 확인 될 경우 Pseudomonas 균을 생각해야 한다. Ciprofloxacin 과 같은 anti-pseudomonal antibioctics (퀴놀론 경구제)로 투여 시작한다. 만일 5~6일 사용했음에도 반응이 느리거나 감염이 반복될 경우 second antipseudomonal drug 로서 IP ceftazidime (not single – 3세대 세파는 단독으로 사용하면 내성이 생기기 때문에 퀴놀론과 같이 사용.), Aminoglycoside, Cefepime, Piperacillin, Imipenem-cilastatin, Meropenem 등을 사용할 수 있다. (Gram negative 보통 3주 이상 치료한다.)
도관 제거의 indication 은 exit site infection 에 peritonitis 가 동시에 발생하였을 경우, catheter infection 이 peritonitis 를 유발하였을 경우, catheter infection 이 해결되지 않을 경우 이다. (치료 실패의 기준은 effective antibiotics 를 3주 이상 사용했음에도 반응이 없는 경우이다.) peritonitis 가 없는 refractory exit-site 또는 tunnel infection 의 경우 항생제 투여하에 도관의 제거와 삽입(새로운 곳)을 동시에 시행할 수 있다. 하지만 Peritonitis 가 동반된 exit-site infection 인 경우 도관을 제거하고 적어도 2주 뒤에(effective antibiotics 투여가 적어도 2주 이상) 증상이 완전히 좋아졌을 때 reinsertion 을 시행한다. fungal peritonitis 라면 더 이 후에 제거한다. re-insertion 은 adhesion 을 직접적으로 볼 수 있는 laparoscopic or mini-laparotomy approach 로 시행한다.
* 복막 투석액이 turbid 하다면, 복막투석액 주머니 뒤의 글자가 보이지 않는다.
CAPD peritonitis
많은 환자들이 다시 PD를 할 수 있으나, PD를 다시 시작하게 되었을 때 ultrafiltration problem 이 흔하게 나타난다.
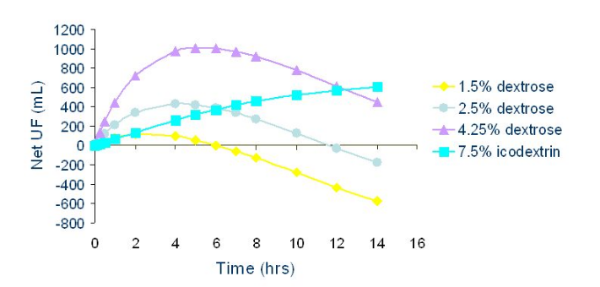
- Glucose % 를 올릴 수록 UF 가 많아진다.
- Exchange frequency (Dwelling time 을 감소) 를 증가시키면 UF 가 많아진다.
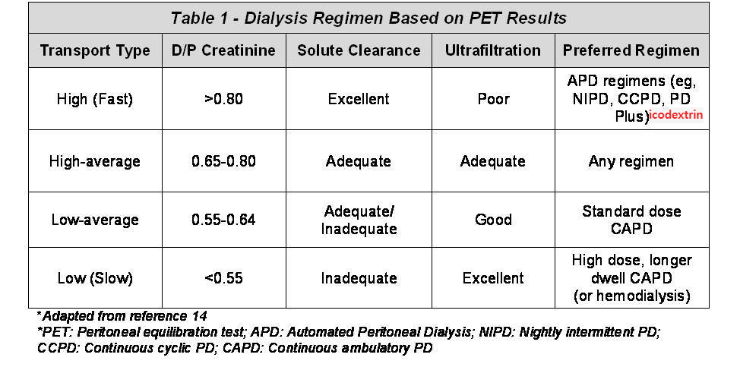
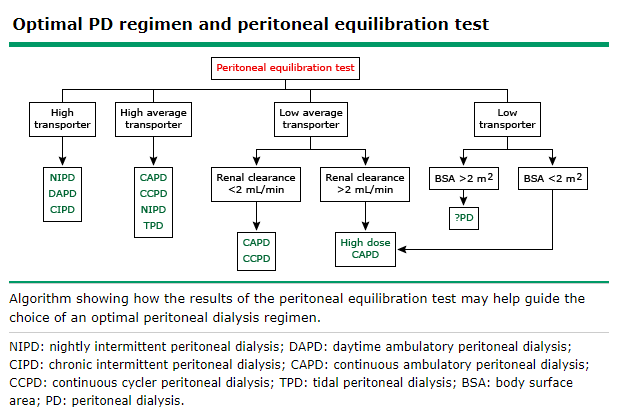
PET test (Peritoneal Equillibration Test)
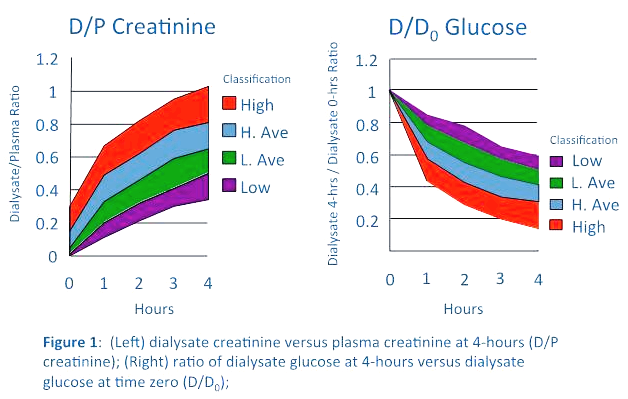
2.5% 2L 를 배안에 넣었다가 (Overnight 8~12 hrs dwell) 0시간, 2시간, 4시간째 Dialysate/Plasma Cr ratio 및 2시간, 4시간째 D/D0 Glucose 를 측정한다. 처음 복막액에는 Cr 이 없다가 시간이 갈수록 혈액에서 복막액쪽으로 Cr 이 빠져나온다. 시간이 지나면서 Dialysate 의 Cr 이 증가한다. 또한 시간이 갈 수록 Dialysate 의 Glucose 가 재흡수 된다. 즉 high transporter 는 Cr 이 복막액쪽으로 빨리 빠져나오고 (빨리 증가), Glucose 는 빨리 재흡수되어 없어진다. high transporter 이면 Solute 제거는 잘 될 지 몰라도, UF 가 제대로 되지 않는 문제가 생긴다. Volume control 이 안되면 Cardiovascular complication 이 증가하여 사망률도 높아지게 된다.
Modified PET test
4.25% dialysis solution infusion 을 사용하여, 0시간, 4시간의 D/D0 glucose, D/P Cr ratio 을 측정한다. 또한 4시간동안 UF 가 400ml 미만이면 UF failure 이다.
UFF & Membrane dysfunction
* High transporter
- Type I UFF –> Volume overload –> Poor survival
원인은 오래 복막투석을 해서 (3년 이상), Glucose 를 많이 써서 (복막이 망가져서), Systemic inflammation (including uremic inflammation), 투석막의 bioincompatibility (low pH, Lactate, Toxic GDP), 복막염이 자주 와서 (너무 자주걸려 EPS (encapsulating peritoneal sclerosis) 발생시 low transporter 가 된다.) 등이 원인이 된다.
* Low transporter
- Type II UFF –> Reduced solute clearance
- EPS 등으로 인해 (Adhesion, fibrosis) peritoneal area 가 감소하여 발생한다.
* Normal range transporter
- Type III UFF –> Increased lymphatic absorption
- Aquaporin deficiency
* Umbilical hernia 가 있어 surgical repair 를 시행하기로 하여 시행한 후 PD를 지속하기 위한 protocol
- 1. Hold PD for 24~48 hrs
- 2. 2 weeks : lower volume, supine PD with dry day
- 3. 2 weeks : lower volume day exchanges
- 4. Full dose PD therapy at 4~5 weeks
* Intra-abdominal Pressure lowering Maneuver
- 1. Bed rest in supine position
- 2. Decreasing exertional activity
- 3. Aggressive cough & constipation management
- 4. Temporary HD
- 5. Low Pressure PD
- Low volume dialysate during day exchange
- Low volume supine PD with/without dry day
- Low volume supine rapid cycling (x6) PD
- Low volume APD – night cycler with dry day