결석의 종류
약 80% 의 환자들의 요석은 calcium stone 으로 되어 있고, 그 중에서도 Calcium oxalate 가 가장 많고, 드물게는 calcium phosphate 가 있다. 그 외 uric acid, struvite (magnesium ammonium phosphate), cystine stone 이 있다. 같은 환자에서 mixed stone 이 있는 경우도 있다.
Calcium stones
대부분 calcium oxalate 으로 구성되어 있다. calcium phosphate stone 은 calcium oxalate stones 과 risk factor 가 비슷하다. (calcium phosphate stones are associated with higher urine pH but not high urine oxalate 를 제외하고)
* Risk factors for calcium stones
(1) Higher urine calcium, with or without hypercalcemia
(2) Higher urine oxalate
— major risk factor for calcium oxalate stone formation
— inflammatory bowel disease, malabsorptive states, or primary hyperoxaluria 와 관련되어 있다.
(3) Lower urine citrate
— can be marked in patients with chronic metabolic acidosis (acidemia 없는 환자도 많은 비중을 차지하고 있음.)
— Citrate is an important inhibitor of calcium oxalate and calcium phosphate stone formation
(4) persistently alkaline urine pH
— can be seen with type I (distal) renal tubular acidosis) + acid load 후에도 발생 가능.
— associated with a higher likelihood of calcium phosphate stone formation
(5) Lower urine volume
— 농도를 높인다.
* Predisposing conditions
(1) Primary hyperparathyroidism
— 반면 Secondary hyperparathyroidism does not increase the risk of stone formation
(2) Medullary sponge kidney
— Medullary sponge kidney is a congenital disorder characterized by malformation of the terminal collecting ducts in the pericalyceal region of the renal pyramids. This collecting duct dilatation, or ectasia, is associated with the formation of both small (microscopic) and large medullary cysts that are often diffuse but do not involve the cortex.
— benign 으로 여겨지나 nephrolithiasis and urinary tract infections 발생할 수 있고, 이러한 합병증이 드물게는 CKD 와 renal failure 로 이어질 수 있다.
(3) Distal (type 1) renal tubular acidosis
— urine pH is persistently high –> medullary nephrocalcinosis를 유발하며, 알칼리이므로 have lower urine citrate levels 를 보인다.
(4) Inflammatory bowel disease, short gut syndrome, bowel resection, or gastrointestinal bypass surgery
— increasing urinary oxalate (due to increased gastrointestinal absorption) and reducing urinary citrate (due to gastrointestinal loss of alkali) 로 인해 calcium oxalate stone 이 현저히 많이 생긴다.
Uric acid stones
Pure uric acid stones occur principally due to a persistently acid urine (pH less than 5.5)
산성인 소변에서는 uric acid 의 침전을 가속화시킨다. (Chronic diarrhea 시 장으로 bicarbonate loss 가 발생하여 acid urine 이 나올 수 있다. )
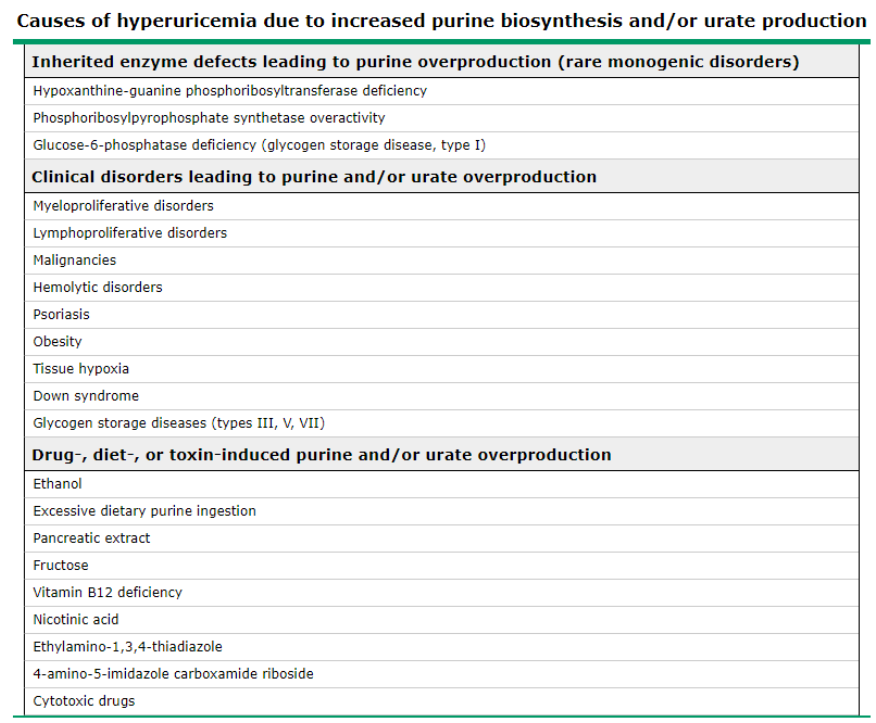
또한 uric acid overproduction 하는 경우에서도 잘 생긴다.
* Uricosuric drugs 는 일시적으로 소변의 uric acid 를 높이긴 하지만, 결국 혈액 내의 요산을 낮추므로 새로운 평형이 맞춰지게되어 uric acid stone 이 잘 생기지는 않는다. (장기적으로 요산 결석 생성의 위험은 없음.)
당뇨와 대사증후군 : both diabetes and the metabolic syndrome are characterized by higher body weight, which is associated with both a more acid urine pH and higher urinary uric acid excretion and supersaturation in proportion to the body mass index.
Struvite stones
chronic upper urinary tract infection due to a urease-producing organism such as Proteus or Klebsiella
magnesium ammonium phosphate crystals 이 urine sediment 에서 보인다.
적절하게 치료하지 않으면 수주에서 수개월 내로 급속하게 커지므로 can develop into a staghorn or branched calculus involving the entire renal collecting system
Cystine stones
only develop in patients with cystinuria (an autosomal recessive disorder)
요로결석의 대사적 원인 분석 방법
병력 청취
식이 습관을 조사해봐야 한다.
– Low fluid intake or a high fluid loss (땀 많이 흘리거나 설사 등)
– A very high animal protein diet (칼슘과 요산 배출이 많아지고 반대로 소변의 구연산은 적어진다.)
– Higher sodium diet (소변의 칼슘 배설이 많아진다.)
– Increased intake of higher oxalate-containing foods (특히 시금치)
– Lower calcium intake (음식내 oxalate 섭취를 증가시켜 결국 소변으로의 oxalate 배출이 늘어난다.)
– Excessive vitamin C and D supplementation
– Excessive sugar (sucrose and fructose) intake (칼슘과 oxalate 배설이 늘어날 수 있다.)
Laboratory testing
* THE COMPLETE METABOLIC EVALUATION
혈액검사 :
Measurement of serum calcium (+ ionized Ca, Albumin), serum bicarbonate 포함한 혈액검사
필요시 intact parathyroid hormone 도 검사 필요. (vitamin D (25(OH) D), TFT 도 필요할 것 같음.)
* 참고로 1,25(OH)2 D의 경우 반감기가 짧아 hypercalcemia 의 진단적인 검사로서 사용하지는 않는다.
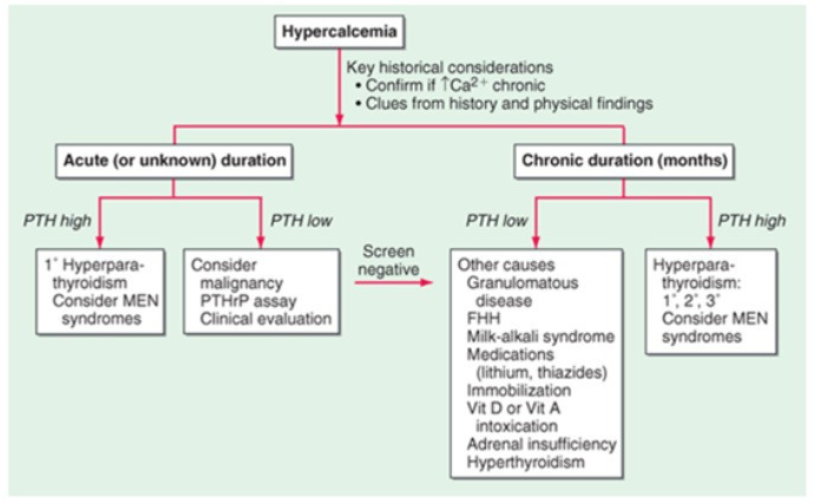
* Familial hypocalciuric hypercalcemia (FHH) 는 CaSR (Calcium-sensing receptor) 의 mutation로 인해 발생하며, FECa (UCCR) 이 <0.01 이면 의심해보아야 한다.
소변검사 :
Urinalysis (urin sediment 와 pH 도 확인)
Urine calcium-creatinine ratio : 정확하지 않기 때문에 추천하지 않는 경우가 있음. 차라리 24시간 소변 수집으로
24-hour urine collections
– urine volume, pH, and excretion of calcium, uric acid, citrate, oxalate, sodium, potassium, and creatinine (to assess the completeness of the collection)
* Measurement of sodium excretion is also important. Higher sodium intake can contribute to increased calcium excretion and will affect the response to a thiazide diuretic when prescribed to reduce urine calcium.
* 소변검사에서 정상 범위의 기준 제시
(A variety of definitions for “normal” are used by different laboratories for each of the urinary parameters)
– Calcium : less than 200 mg (5.0 mmol) per day in women or less than 250 mg (6.25 mmol) per day in men
– Uric acid : less than 750 mg (4.5 mmol) per day in women or less than 800 mg (4.8 mmol) per day in men
– Oxalate : less than 40 mg (0.44 mmol) per day in both women and men
– Citrate : greater than or equal to 450 mg per day in both women and men
검사 결과에 따른 대책
소변에서 칼슘이 높다면
— primary hyperparathyroidism, sarcoidosis, and distal (type 1) renal tubular acidosis 인지 생각해보자
— thiazide 등을 써야할지 생각
소변에서 구연산이 낮다면
Supplementing alkali intake (eg, potassium citrite or potassium bicarbonate) will increase urinary citrate excretion.
단 소변 pH 가 6.5 이상이라면 citrite 보충은 조심해야한다. (calcium phosphate 가 주된 성분이라면, citrite 같은 alkali 보충은 bicarbonte 로 대사되어 stone 형성을 더욱 가속화할 수 있다.
소변에서 oxalate 가 높다면
low-oxalate diet 를 우선 시도해본다. (시금치, 감자, 아몬드 등을 피한다.)
urine calcium 이 낮다면, 식이로 섭취되는 칼슘을 증량한다.
소변에서 요산이 높다면
저퓨린식이 및 체중 감소를 시도한다. 단, 소변의 pH 가 6.0 보다 크다면, high urine uric acid 라고 해서 stone 형성에 크게 기여하지 않았을 것이다.
소변의 양이 적다면
수분 섭취를 늘려 하루에 2L 이상은 소변 보도록 한다.